在ELCC会议的“TKI和其他治疗方式联合治疗(Combining TKI with other strategies)”专场,法国里昂中心医院(Centre Hospitalier Lyon-Sud)放疗科 Francoise Mornex教授介绍了TKI和放疗的联合治疗策略。
在ELCC会议的“TKI和其他治疗方式联合治疗(Combining TKI with other strategies)”专场,法国里昂中心医院(Centre Hospitalier Lyon-Sud)放疗科 Francoise Mornex教授介绍了TKI和放疗的联合治疗策略。
Mornex教授指出,III期非小细胞肺癌(NSCLC)是异质性、难以治疗的疾病,或需要个体化治疗策略。其最佳放疗和化疗方案还不确定,放疗联合靶向疗法±化疗有一定的合理性。靶向药物与放疗联合的生物学效应(biological effect)是1+1=2、1+1<2还是 1+1>2?目前我们需要明确使用哪种靶向药物,何时使用,以及如何评估这种联合治疗的效果。
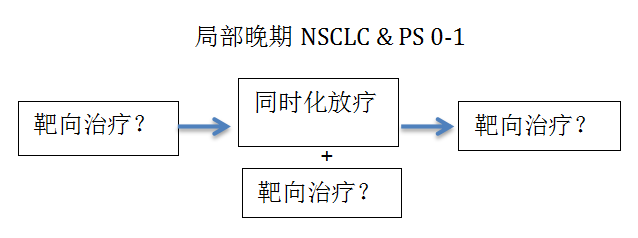
局部晚期NSCLC患者的治疗流程如下
根据目前的研究,对于EGFR突变阳性的III期NSCLC患者,根据分子诊断结果的选择放疗和靶向药物的联合治疗策略是可行的。吉非替尼/厄洛替尼+放疗的研究结果目前令人失望,未来的研究方向是个体化的联合治疗策略,比如根据基因检测结果选择放化疗(Genetically-targeted chemoRT)。在抗肿瘤血管生成治疗方面,西妥昔单抗联合放疗是有前景的组合。贝伐珠单抗联合放疗似乎是危险的组合,在目前的研究中没有改善患者的OS和PFS(相比单用放化疗)。不建议抗VEGF治疗联合SABR,抗VEGF治疗与放疗的联合需要优化,相比单用放疗治疗寡转移肿瘤,加用舒尼替尼(sunitinib )增加≥3级毒副作用的发生率,建议减少25%的剂量(50mg 降低到37.5 mg)。BRAF抑制剂vemurafenib联合放疗被用于治疗黑色素瘤(Anker et al. JCO 2013)。放疗是重要的抗血管生成因素。
目前为止,III期NSCLC患者中TKI和放疗联合治疗策略的研究没有阳性结果,个体化的联合治疗策略或可改进治疗效果。正在进行的和未来即将开展的试验中,一些新药显示良好的前景,比如放疗联合nivolumab的研究(RTOG Foundation),新型PARP抑制剂veliparib联合放疗和化疗(卡铂、紫杉醇)治疗III期NSCLC患者的研究(NCT02412371)。III期NSCLC患者加用放疗增加放疗相关毒性。目前不能在临床中常规使用靶向和放疗的联合治疗策略,亟需临床前模型。
在《肿瘤瞭望》的采访中,Mornex教授指出,放疗和靶向疗法联合是一个重要课题,也是一个比较新的课题。放疗和靶向药物联合既复杂又困难,这种组合治疗一定要增加疗效而无危害性。在某些情况下,这种联合治疗策略非常容易、有用;在某些情况下,这种联合治疗策略很困难,会增加治疗毒性,引起不能耐受的副作用。所以在联合放疗和靶向药物治疗患者之前,我们必须确保有足够的研究数据,了解这种组合策略的并发症。Mornex教授特别关注放疗+抗血管生成药物联合方案的耐受性,这种治疗策略可导致正常组织发生瘘管、出血等并发症。
放疗本身会引起机体的免疫变化,原发肿瘤放射治疗有时可减轻远处肿瘤进展。因此,Mornex教授对放疗和免疫疗法联合治疗的免疫效应非常感兴趣,特别期待这一领域的研究进展。
对于有驱动基因的晚期NSCLC患者,局部治疗的地位如何?Mornex教授认为,对于有驱动基因的晚期NSCLC患者,局部治疗仍然是新兴的领域,但也是未来治疗策略的一部分。大多数患者确诊后会选择疗效好的靶向治疗,局部治疗对于局部控制和提高生存率非常重要。目前有两种重要的局部治疗方法:手术和立体定向放射治疗,应根据患者自身情况、肿瘤的位置、患者病史和治疗环境等因素从中选择,立体定向放射治疗是有效的、非侵入性的治疗,手术在需要组织样本、或放疗与靶向药物联合会导致无法忍受毒性等情况下是更好的选择。局部治疗是提高患者的预后的重要方式。
Oncology Frontier:You have an report on combining TKI with radiotherapy in locally advanced disease, would you please give us the main points of the report?
《肿瘤瞭望》:您在ELCC会议上的报告是“TKI和放疗联合治疗局部晚期非小细胞肺癌”,能否请您简单介绍报告的核心内容?
Dr Mornex: It is an important topic and quite a new topic, which will have more and more impact in the future. The method of combining radiation and targeted agents is complex and difficult and very important in terms of the implications because radiotherapy is an efficient technique and targeted agents are very efficient in most cases and their combination must increase this efficacy without jeopardizing tolerance. According to the different agents, in some situations it is very easy and helpful to combine them. In other situations, it is more difficult due to increased toxicity which can induce intolerable side effects, so we have to be sure we have enough data in the literature before using those combinations. I am especially concerned about the reduced tolerance that can potentially occur in combinations between radiation and the antiangiogenic agents, which are extremely powerful (and probably too powerful) against normal tissues inducing fistulae, hemorrhage and other complications. So it is very important to be aware of these complications and to be aware of the available clinical trials before prescribing these combinations.
Mornex教授:放疗和靶向疗法联合是一个重要课题,也是一个比较新的课题。放疗和靶向疗法联合复杂而有困难,这种组合治疗一定要增加疗效而无危害性。在某些情况下,这种联合治疗策略非常容易、有用;在某些情况下,这种联合治疗策略很困难,会增加治疗毒性,引起不能耐受的副作用,所以在联合放疗和靶向药物治疗患者之前,我们必须确保有足够的研究数据,了解这种组合策略的并发症。我特别关注放疗+抗血管生成药物联合方案的耐受性,这种治疗策略可导致正常组织发生瘘管、出血等并发症。
Oncology Frontier: Would you please talk about the role of local therapies in advanced molecular-driven NSCLC?
《肿瘤瞭望》:对于有驱动基因的晚期NSCLC患者,局部治疗的地位如何?
Dr Mornex: It is a very interesting topic which is still emerging but will be part of our treatment strategies in the future. Most of our patients present with metastatic disease at first diagnosis. They are treated with targeted agents which are powerful, but despite this efficacy, local therapy is still important and is now very efficient in terms of local control and improving survival. We have two kinds of treatment at our disposal – surgery and stereotactic radiation. According to the patient, the location of the tumor, the history of the patient and the characteristics of the therapeutic environment, we have good arguments to choose either stereotactic radiation as a powerful and non-invasive treatment, or surgery, which may be preferable in certain situations such as when we need histological samples or in those situations where the combination of radiotherapy with the targeted agents would cause an intolerable toxicity. So we have powerful local treatments and the choice of which to use in order to improve outcomes for patients.
Mornex教授:对于有驱动基因的晚期NSCLC患者,局部治疗仍然是新兴的领域,但也是未来治疗策略的一部分。大多数患者确诊后会选择疗效好的靶向治疗,对于局部控制和提高生存率非常重要。目前两种重要的局部治疗方法:手术和立体定向放射治疗,我们根据患者自身、肿瘤的位置、患者病史和治疗环境等因素从中选择,立体定向放射治疗是有效的、非侵入性的治疗,手术在需要组织样本、或放疗与靶向药物联合会导致无法忍受毒性等情况下是更好的选择。局部治疗是提高患者的预后的重要方式。
Oncology Frontier: ELCC 2016 released the results of a number of studies, ?which study are you most interested in?
《肿瘤瞭望》:ELCC 2016 发布了多项研究成果,您对哪项研究最感兴趣?
Dr Mornex: The field that is extremely important is the field of immunotherapy. This field is large and improving and I am deeply interested in the combination of radiation and targeted agents, specifically the combination of radiation and immunotherapy. Radiation by itself induces immune changes in the body and in a few situations is able to decrease the progress of a tumor far away from the primary tumor which has been irradiated. So the combination of the immune effect of radiation and immunotherapy is a fascinating field and I look forward to results in this field especially.
Mornex教授:我最感兴趣的免疫治疗领域的研究。我对放疗和靶向药物联合治疗深感兴趣,特别是放疗和免疫治疗相结合。放疗本身会引起机体的免疫变化,原发肿瘤放射治疗有时可减轻远处肿瘤进展。因此,我对放疗和免疫疗法联合治疗的免疫效应非常感兴趣,特别期待这一领域的研究。






 京公网安备 11010502033352号
京公网安备 11010502033352号